SMART Surgery Technique (Samadi Modified Advanced Robotic Technique)
Having completed fellowship training in both urologic oncology and laparoscopy, Dr. Samadi’s technique as described below builds on oncologic principles learned with open radical prostatectomy and transferred to a robotic approach. In the technique, he recreates the classic open anatomic RRP technique as closely as possible on the robotic platform. He does not view the robot as a good unto itself, but, rather, as a tool that permits enhanced anatomic radical prostatectomy by improving vision and allowing angles of dissection not possible with open or straight laparoscopic instruments.
The SMART Technique
It should be emphasized that the SMART technique is an advanced technique that should not be performed early in a novice robotic surgeon’s learning curve. Since 2003, Dr. Samadi has performed over 2,000 RALPs, approximately half by this technique. In the 12 months since the final modifications were made to this technique in early 2008, he has performed more than 2,224 RALPs.
The below video explains the underlying principals of the SMART surgery technique and the benefits it provides:
The SMART Surgery Technique, as described below, can be performed in a mean operative time of less than 2 hours.
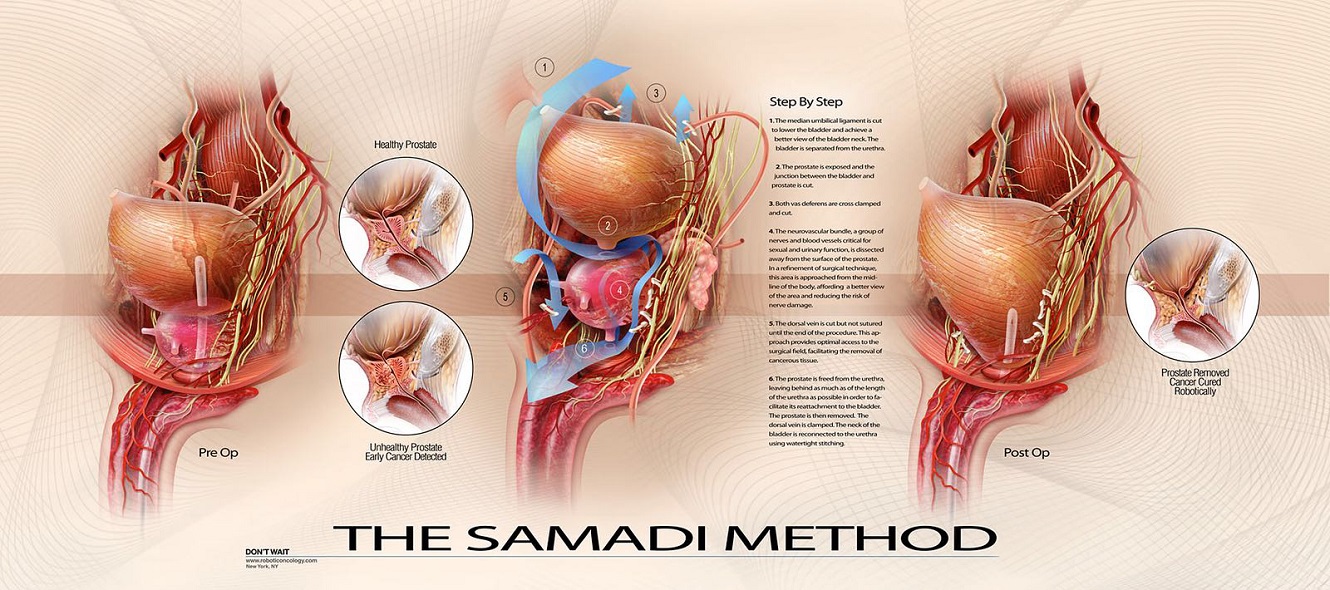
By means of this advanced surgery for prostate cancer, three important goals are achieved:
- Total cancer removal
- Sexual potency
- Urinary continence
Treatment trifecta is an important characteristic of the SMART Surgery Technique.
These are the 8 important steps of SMART surgery:
Step 1: Dropping the bladder
The medial umbilical ligaments are coagulated and transected bilaterally and the incision is carried down to the vasa deferentia. The space of Retzius is developed bluntly. Fat on the anterior surface of the prostate is excised and included with the permanent prostate specimen. This fat is sent for pathological analysis after recent findings demonstrated that it occasionally harbors lymph nodes, which, when positive, portend poor prognosis (Urology 2007; 70:1000-3).
Step 2: Bladder neck transection
Once the prostate is exposed, the bladder neck is identified and the medial aspect of the bladder neck incised with electrocautery until the Foley catheter is exposed. The catheter is grasped with the fourth robotic arm and retracted anteriorly. Note that the endopelvic fascia remains intact at this point and the DVC is not ligated.
Step 3: Posterior bladder neck transected
The posterior aspect of the bladder is now exposed and a median lobe or TUR defect should be apparent if present. (Management of median lobes can be quite complex, and is outside the scope of this discussion.) The posterior aspect of the bladder neck is transected with electrocautery, while keeping in the same plane as the anterior bladder neck dissection.
Step 4: Seminal vesicle (SV) dissection
Given the proximity of the nerve erigentes of Walsh to the tips of the seminal vesicles, their dissection should be performed without cautery. The vas deferens is dissected several centimeters distally, which facilitates the delivery of the remainder of the SV. Once in the correct plane and the glistening white of the vas is exposed, the thin layer of connective tissue covering the SV is bluntly dissected posteriorly as the SV is pulled anteriorly. After the entirety of the SV has been exposed, the artery to the SV should be seen entering laterally, where it is clipped distally and transected. We prefer the articulation afforded by the robotic Hem-o-Lok clip applier (Weck Closure Systems, Research Triangle Park, NC). Once one SV has been dissected, it is retracted anteriorly to facilitate the dissection of the contralateral SV.
Step 5: Posterior dissection/nerve spar sparing/ EPF incision
Following dissection of bilateral SVs, the SVs are grasped with the fourth robotic arm, retracted superio-laterally, and rotated away from the side of nerve sparing (to the left and counter-clockwise for right-sided nerve sparing). Minimal traction is thus placed on the neurovascular bundles. It should be emphasized that from this point onward, all dissection and nerve sparing are performed with blunt dissection, using the curved robotic scissors. No cautery is used at any point. (In the event of significant disease burden prohibitive of nerve sparing, the neurovascular bundle is excised widely with a standard lateral incision of the endopelvic fascia.)
The posterior aspect of the prostate is dissected bluntly in antegrade fashion for several centimeters and the prostatic pedicle is exposed. The large urethral branches are controlled using a robotically applied Hem-o-lok clip. Starting at the lateral aspect of the SV, interfascial nerve sparing is performed in an antegrade fashion from the 5 o’clock to the 2 o’clock position on the prostate, similar to the “veil” or “curtain” technique. Small capsular branches of the pedicle are controlled with small metal clips applied robotically.
Care should be taken to visualize the ureteric orifices prior to reconstruction and to avoid their inclusion in the sutures. Once the endopelvic fascia has been released anteriorly for several centimeters at the 2 o’clock position, a robotically applied Hem-o-lok clip is placed on the lateral fascia parallel with the plane of dissection to control tributaries of the DVC. The fascia is then incised with the cold scissors. This proceeds in an antegrade fashion until the apex is dissected and the DVC exposed. The fourth robotic arm is then shifted to the right side and rotated in a clockwise fashion to set up the left-sided nerve sparing.
Step 6: DVC/Apical dissection
After both neurovascular bundles have been spared to the apex, the pneumoperitoneum is temporarily increased to 20 mm Hg. The anesthesiologist is instructed to carefully monitor end tidal CO2. The DVC and puboprostatic ligaments are cut with cold scissors as the prostate is retracted superiorly and rotated anteriorly as in open RRP. The apex of the prostate, urethra, and neurovascular bundles can easily be visualized and dissected free. Minimal suction is used during this step to minimize blood loss from the open DVC. The urethra is dissected circumferentially and cut with cold scissors to leave as long a urethral stump as possible, maintaining the striated sphincter.
After the specimen is removed and bagged, the DVC is oversewn with a running 3-0 polyglactin suture on an SH needle, taking care to avoid the dissected neurovascular bundles. Arterial and venous bleeding is easily controlled with this suture, without distorting the anatomy of the urethra or sphincter. The pneumoperitoneum is returned to 15 mm Hg as soon as possible. Blood loss for this portion of the procedure is rarely more than 50 mL. Arteries are often present at the 11 and 1 o’clock position, which can be coagulated with bipolar cautery if bleeding is excessive. In the rare instance when bleeding is excessive, the DVC can be oversewn in running fashion prior to removal of the specimen.
Step 7: Bladder neck reconstruction
The bladder neck is reconstructed with a posterior tennis-racket closure with a running 2- 0 polyglactin suture on a CT needle, as described for open RRP. Care should be taken to visualize the ureteric orifices prior to reconstruction and to avoid their inclusion in the sutures. The bladder neck is narrowed to the caliber of an 18F catheter. Fat on the anterior surface of the prostate occasionally harbors lymph nodes, which when positive portend poor prognosis.
Step 8: Urethrovesical anastomosis
Using the technique of van Velthoven, two 3-0 Monocryl sutures on UR-6 needles of different colors are tied together and run circumferentially around the urethral-vesical anastomosis. The exaggerated curve of the UR needle facilitates accurate placement of sutures in the reconstructed bladder neck. We do not advocate the use of posterior fascial reconstruction prior to the anastomosis because randomized evidence has demonstrated its inefficacy (J Urol 2008; 180:1018-23).